
Adolescent tobacco and nicotine use in the DRC

Adolescent use of tobacco is a significant public health issue worldwide, with about 37 million individuals aged 13–15 years currently using tobacco.
In the Democratic Republic of Congo (DRC), youth tobacco and nicotine use emerges as a national concern. In 2014, the DRC ranked as the third-highest African country for current adolescent tobacco use. Urbanization, peer influence, targeted advertising, and weak regulations are causes of early initiation.Adolescent tobacco and nicotine use is linked to a myriad of health problems; these include an increase in the number and severity of respiratory illnesses, cardiovascular diseases and cancer, decreased physical fitness, and potential effects on lung growth and function. Indeed, adolescent smokers are more likely than non-smokers to have panic attacks, anxiety disorders, and depression. In fact, tobacco-related diseases kill about 100 adolescents annually in the DRC, while long-term users lose over a decade compared to non-users. Tobacco control among children and adolescents is therefore important, because it reduces the risks of a range of diseases and adolescents’ chances of taking up smoking themselves. Equally, avoiding tobacco exposure allows children to grow up free from its dangers, which is a key aspect of providing clean, safe, and secure environments.
This page presents data related to the consumption of tobacco and/or nicotine products among adolescents aged 10–17 years in the DRC. The tobacco products include manufactured cigarettes, roll your own (RYO) cigarettes, shisha, smokeless tobacco products (STPs), and heated tobacco products (HTPs). The nicotine products are electronic cigarettes (e-cigarettes) and oral nicotine pouches.
Using findings from the Data on Youth and Tobacco in Africa (DaYTA) survey conducted by Development Gateway: An IREX Venture in partnership with Research Initiatives for Social Development (RISD) and Laboratory for Survey and Research for Development (SRD Lab) in 2024, this page explores key data, current trends, underlying factors of youth tobacco and nicotine consumption, tobacco and nicotine marketing strategies, and cessation activities in the DRC. Detailed methodological information about this survey can be found in the Methods section and is accessible here. The fact sheet and full country report can be accessed here and here, respectively.

Prevalence of useof any tobacco and/or nicotine products
This module explores the prevalence of tobacco and nicotine products, highlighting both traditional forms such as manufactured cigarettes and RYO cigarettes, and emerging products like shisha, e-cigarettes, and nicotine pouches.
Findings from the 2024 DaYTA study
suggest that nearly 1 in 5 adolescents (18.5%) have ever tried a tobacco or nicotine product, and more than 1 in 10 (11.9%) are current users of any tobacco or nicotine product (representing about 5.08 million and 3.27 million adolescents respectively, on a general adolescent population of 27.5 million individuals). This underscores the pressing need for targeting prevention, particularly as both conventional and new-era products become increasingly popular among adolescents.Overall prevalence of tobacco and nicotine product use among adolescents aged 10-17 years in the DRC
Source: DaYTA DRC (2024)
To deepen our understanding of the consumption of tobacco and/or nicotine products among adolescents in the DRC, we disaggregate data by sex, age, school attendance, and residence, among other factors, using tobacco and nicotine current use values exclusively.

Prevalence by sex of current tobacco and/or nicotine product use
The disparity in any tobacco and/or nicotine product consumption between Congolese boys and girls is significant. Indeed, the prevalence among girls (7.1%) is less than half the rate for boys (16.2%).
This pattern is similar to the average rate of tobacco use in the WHO African region, where tobacco use among girls is 1.5 to 4 times lower than that of boys. Similar results are also found in broader African studies.It should be noted that, for all product categories (smoked tobacco, smokeless tobacco, heated tobacco, and nicotine pouches), the prevalence was higher among boys than girls, except for e-cigarettes, where only one-fifth of the users were boys.
Prevalence by sex of current tobacco and/or nicotine product use among adolescents aged 10-17 years in the DRC

Prevalence by age group of current tobacco and/or nicotine product use
Current use of any tobacco and/or nicotine product among Congolese adolescents increases with age. Indeed, while the youngest age group has the lowest percentage (8.9%), the oldest one has the highest prevalence (18.9%).
This pattern aligns with other research and reports that show increasing use with age. This trend is observed for all tobacco products, but fails to be the case for nicotine products where adolescents aged 13-15 years are the least consumers.Prevalence by age group of current tobacco and/or nicotine product use among adolescents aged 10-17 years in the DRC
Source: DaYTA DRC (2024)
Prevalence by residence of current tobacco and/or nicotine product use
Despite the intensification of anti-smoking programs and campaigns in cities, the current use prevalence of any tobacco and/or nicotine product in the DRC is higher in urban areas (17%) than in rural zones (10.6%).

Prevalence by region of current tobacco and/or nicotine product use
Though the DRC is subdivided into 26 provinces, in the study carried out by DaYTA, group names rather than current administrative provinces are used to capture prevalence by regions. These groups include: Katanga, Kasaï, Léopoldville, Équateur, Orientale, and Kivu.
Of all the regional groups, Kivu records the lowest current use prevalence of tobacco and/or nicotine products (4.4%), while Orientale has the highest prevalence percentage (30.1%). Only the Kivu (4.4%) and Léopoldville (11.1%) regions have prevalence rates lower than the national rate of 11.9%.Regardless of the age considered when studying prevalence of tobacco product use in the DRC, the regional trends remain the same. Indeed, the prevalence pattern for some regions is identical to that obtained from the Multiple Indicator Cluster Survey (MICS) 2017–2018 survey.
The Kivu region, for example, had the lowest prevalence of tobacco consumption among adults aged 15–49 years in the DRC (Nord Kivu (1.09%), Sud Kivu (1.34%), exactly as is the case with adolescents’ data. Similar results are obtained for the Équateur and Orientale regions, where the prevalence of tobacco products among adults aged 15–49 is high, with the provinces of Nord Ubangi (13.14%) and Sud Ubangi (12.5%), all found under the Équateur group, having the highest prevalence.Prevalence by school enrollment status of current tobacco and/or nicotine product use
The prevalence of any tobacco and/or nicotine product consumption is higher among youths not attending school in the DRC (16.4%).
Though overall prevalence indicates that out-of-school adolescents are greatest consumers of tobacco and nicotine products, this is not the case for some specific products. Indeed, for smokeless tobacco, prevalence is higher among adolescents in school (6%) than among those not in school (5.1%). The same is true for heated tobacco products, where smoking prevalence is higher among adolescents in school (0.1%) than among those not in school (0.04%).Prevalence by school enrollment status of current tobacco and/or nicotine product use among adolescents aged 10-17 years in the DRC
Source: DaYTA DRC (2024)
Prevalence by product of current tobacco and/or nicotine product use
Some tobacco and nicotine products, such as shisha or e-cigarettes, are gaining popularity among adolescents in Africa, as many perceive them as “safer” than cigarettes.
The overall prevalence of any tobacco and/or nicotine product among youths in the DRC is high, with 11.9% reporting current use. Tobacco products are more commonly used (11.8%) than nicotine products (0.6%): smoked tobacco has the highest prevalence (8%), while heated tobacco is much less common (0.1%). Pertaining to nicotine products, nicotine pouches (0.6%) are preferred over e-cigarettes (0.04%).The pattern of current tobacco and nicotine use among adolescents worldwide is not the same. In developed countries like the USA, for example,
nicotine products (e-cigarettes 5.9% and nicotine pouches 1.8%) have the highest prevalence, whereas shisha (0.7%) and pipe tobacco (0.5%) are the least consumed. This could suggest a greater exposure of adolescents to emerging products in developed countries than in developing countries.Prevalence by product of current tobacco and/or nicotine product use among adolescents aged 10-17 years in the DRC
Source: DaYTA DRC (2024)
Prevalence of nicotine product use
Nicotine products are the least consumed by adolescents in the DRC, with prevalence values barely reaching 1%.
Of the nicotine products considered during the study, nicotine pouches (0.6%, approximately 165,000 adolescents) are the most used, while e-cigarettes record a very low prevalence of nearly 0%. The report indicates that this high nicotine pouch consumption is justified by the fact that most users were curious about the product and were influenced by peers. The trends in nicotine consumption among Congolese adolescents varies by product type. While boys consume more nicotine pouches than girls (0.8% vs 0.6%), girls consume more e-cigarettes than boys (0.10% vs 0.01%).Prevalence of current nicotine product use among adolescents aged 10-17 years in the DRC
Source: DaYTA DRC (2024)
Nicotine use appears to have an irregular pattern with age. While adolescents aged 16–17 years are the greatest consumers (0.9%) followed by those aged 10–12 years (0.7%), adolescents aged 13–15 years are the least consumers (0.3%).
This trend is quite abnormal but could be justified by some contextual factors like the absence of parents during adolescents’ questioning and independently self-reported values (no use of proxies).
Initiationof tobacco and nicotine products

Initiation age of tobacco and nicotine products use
In the DRC, the average initiation age to tobacco and nicotine consumption ranges between 11 and 14 years. Specific to products, initiation to e-cigarettes is done earliest (11 years). On the other hand, shisha has the oldest average initiation age (14 years). Depending on the type of product, initiation age equally varies by sex. For boys, the average initiation age is latest for shisha (14 years) and earliest for smokeless tobacco and RYO cigarettes (12 years). On the other hand, girls initiate e-cigarettes earliest (10 years), while HTPs and shisha (14 years) have the oldest initiation ages. These initiation ages fall within the range suggested by WHO for the African region.

Reasons for initiating tobacco and nicotine products use
Different factors predominantly drive adolescents’ initiation of tobacco and nicotine product use in the DRC. Factors like having a friend using the products, living in a family where these products are consumed, and curiosity are common for all products.
Peer influence is the leading reason for starting manufactured cigarettes (59.1%), RYO cigarettes (59.3%), shisha (66.1%), and nicotine pouches (32%). In contrast, smokeless tobacco use is mainly influenced by use by family members (47.2%). HTPs is primarily adopted due to emotional distress—with 38.1% of users citing feelings of anxiety, stress, or depression—while curiosity is the main factor prompting the use of electronic cigarettes (18.9%). These results corroborate those obtained by most scientific works.Top five reasons for initiation for tobacco and nicotine product
Source: DaYTA DRC (2024)
With whom during initiation
In the DRC, the social context in which adolescents first use various tobacco and nicotine products varies.
For manufactured cigarettes, RYO cigarettes, shisha products, and nicotine pouches, the most common initiation context was with at least one friend—with 67.6%, 70.0%, 79.7%, and 41.6% of adolescents, respectively, reporting that their first use occurred in a social setting with friends. However, for smokeless tobacco products and e-cigarettes, the highest percentages of initiation occurred with at least one family member (52.3% and 13.0%, respectively). Meanwhile, the predominant context for initiating HTPs was when adolescents were alone, with 58.6% reporting solitary initiation.Who adolescents were with at initiation
Source: DaYTA DRC (2024)

Accessto tobacco and nicotine products
How adolescents obtain tobacco and nicotine products
The channels through which Congolese adolescents obtain tobacco and nicotine products vary by product. While getting the products from someone else is prevailing for all products, for manufactured cigarettes and shisha, the most common method of access was purchasing them at a kiosk, with 46.3% and 39.3% of users, respectively, reporting this channel. In contrast, RYO cigarettes, as well as smokeless tobacco products, HTPs, and nicotine pouches, were most frequently obtained from someone else, with 46.3%, 40.5%, 45.1%, and 33.2% of users, respectively, indicating that this was their main source. E-cigarettes, however, were rarely accessed by adolescents, with the highest reported method being obtaining them from someone else (which accounts for only 0.1% of cases).
How adolescents in the DRC obtain tobacco and nicotine products for initiation
Source: DaYTA DRC (2024)
Places where adolescents use tobacco and nicotine products
Despite bans on the use of tobacco products in public spaces, adolescent Congolese use different tobacco and nicotine products in restaurants, bars, and other open locations. For manufactured and RYO cigarettes, the most common setting was at a friend’s house, reported by 42.5% and 40.4% of users, respectively.
In contrast, shisha products, smokeless tobacco, and e-cigarettes were predominantly used at home—39.7%, 67.7%, and 55.1% of users, respectively. HTPs were most frequently used in public spaces (52.3%), while nicotine pouches were most often used at restaurants (28.6%). Except for manufactured cigarettes, adolescents report using all other tobacco/nicotine products in public places. Equally, shisha is the most consumed tobacco product in bars (29.6%).Places of use – tobacco/nicotine among adolescents
Source: DaYTA DRC (2024)
Adolescents’ tobacco and nicotine purchase refusal because of age
For most tobacco and nicotine products, the majority of adolescents had not tried to buy them within the last 30 days:
63.1% for manufactured cigarettes, 82.4% for RYO cigarettes, 88.1% for shisha, 80.4% for smokeless tobacco, 88.3% for both e-cigarettes and nicotine pouches. The only exception was HTPs, where a striking 83.8% of respondents refused to answer whether they had attempted a purchase. It is important to note that 31.0% of adolescents said that no one refused to sell them manufactured cigarettes.Purchase refusal because of age
Source: DaYTA DRC (2024)
Adolescents’ purchase of single sticks
Evidence from the DaYTA study
suggests that current users of manufactured cigarettes and RYO cigarettes smoke an average of 1 cigarette per day, while adolescent users of both manufactured and RYO cigarettes consume an average of 3 cigarettes per typical smoking day. There is no other smoked tobacco products consumed by adolescents.Congolese adolescents’ purchase of single sticks
Source: DaYTA DRC (2024)

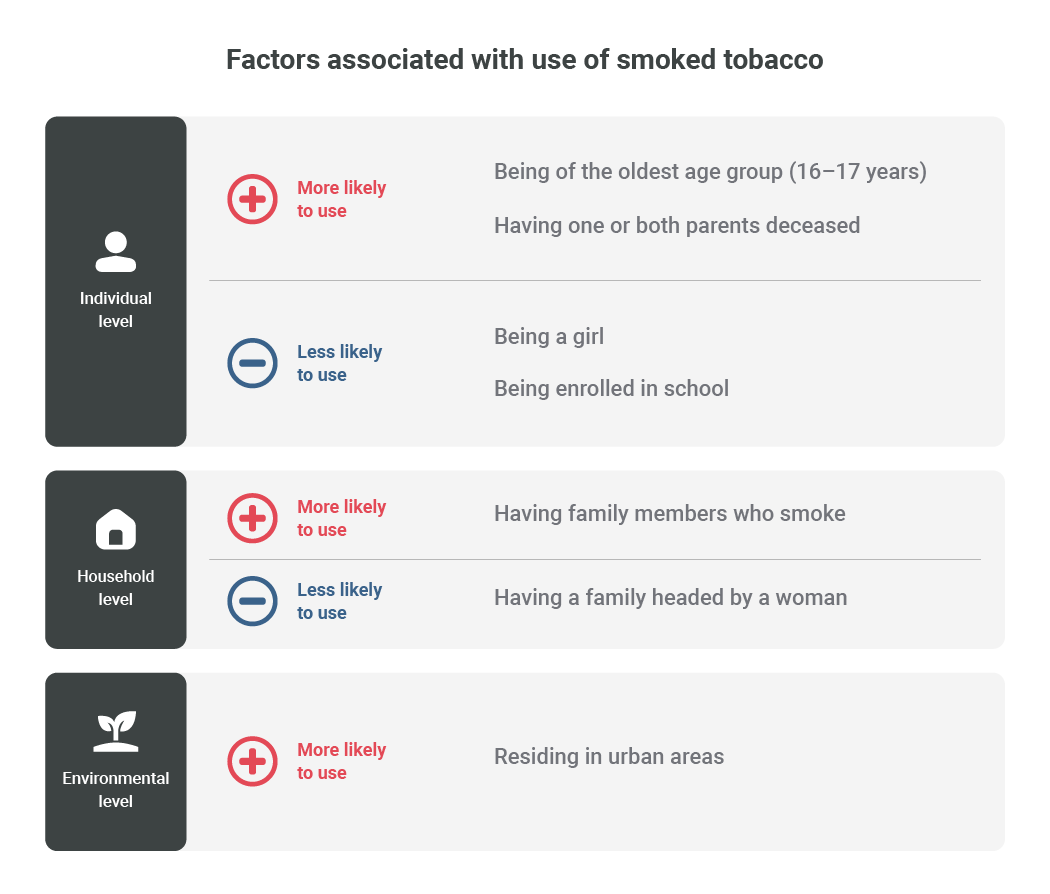
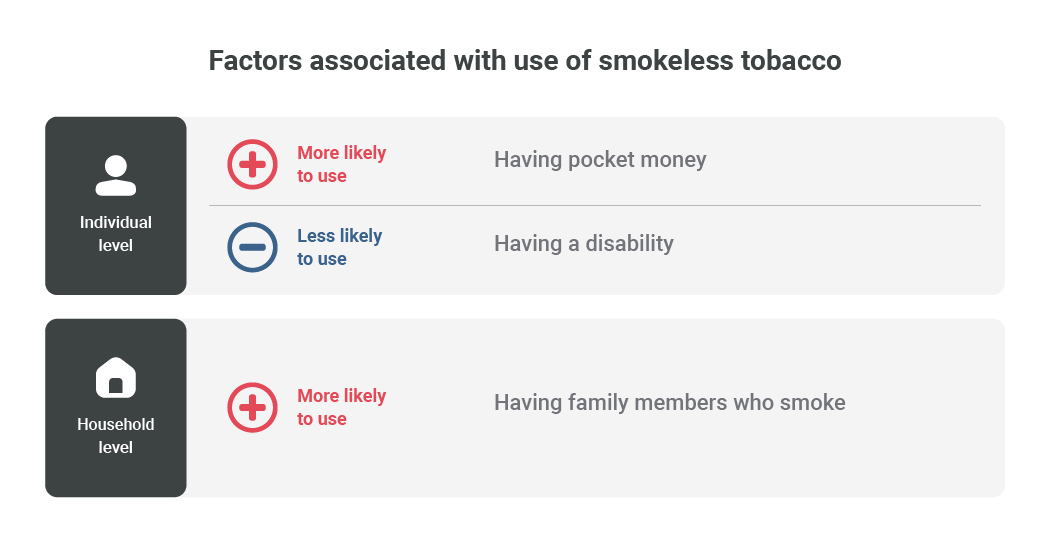
Factors associatedwith tobacco and nicotine use
The DaYTA study considers three groups of factors likely associated with tobacco and nicotine use among adolescents aged 10–17 years in the DRC.
They include: individual-level factors, household-level factors, and environmental factors. These factors are summarized as follows: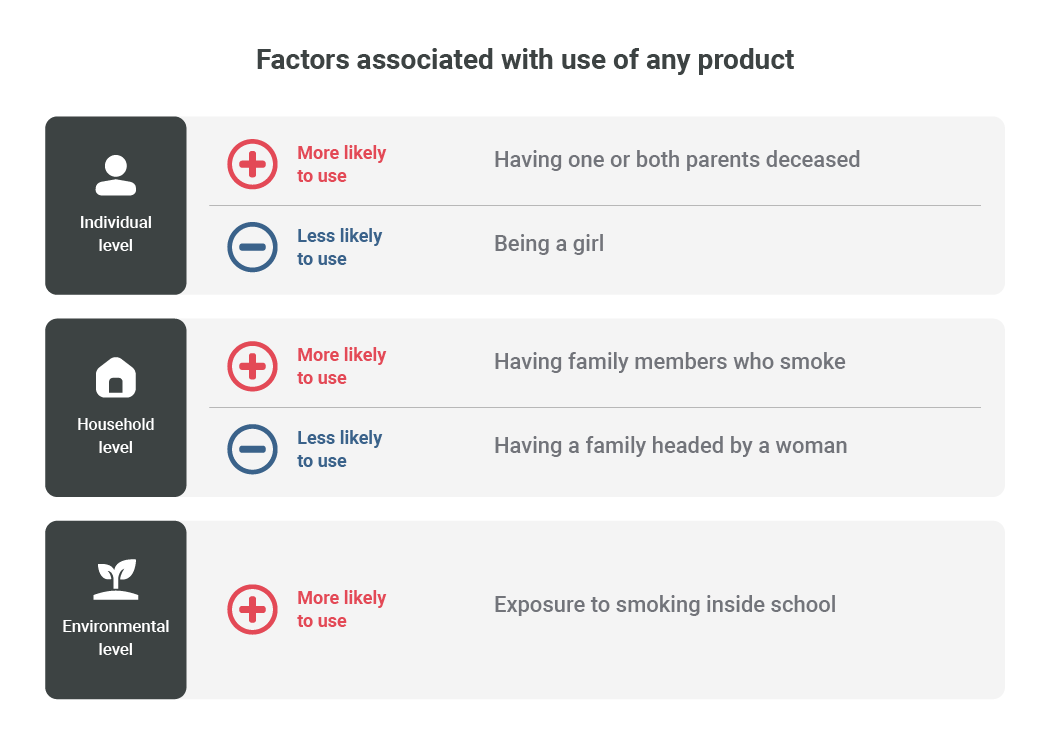

Knowledge, attitude, and perceptionof tobacco and nicotine in the DRC
Knowledge about tobacco harm
Tobacco-related knowledge here refers to all knowledge about the harmful effects of using tobacco products. Overall, 50.7% of Congolese adolescents who reported having ever used a tobacco product demonstrated little knowledge of the health risks associated with tobacco consumption and exposure, while 18% demonstrated no knowledge of the dangers associated with tobacco consumption or exposure.
These results align with those obtained in Nigeria, where 72.3% of study subjects reported having low tobacco-related knowledge.Distribution of knowledge of health risks associated with tobacco use and exposure among adolescent ever-users in the DRC
Source: DaYTA DRC (2024)
Irrespective of the sub-category considered, the largest proportion of the adolescent population aged 10–17 years in the DRC have low knowledge on the health risks associated with tobacco use and exposure.
Disaggregation of knowledge about the health risks associated with tobacco use and exposure among adolescent ever-users in the DRC
Source: DaYTA DRC (2024)
In the DRC, awareness of relatively new tobacco and nicotine products among adolescents is quite low. Only 8.9% of respondents have heard of e-cigarettes, making them the most recognized among three products; HTPs are known to 6.3% of adolescents, while awareness of nicotine pouches is slightly lower at 5.7%.
Attitude towards tobacco and nicotine products
In the DaYTA study,
a “negative attitude” is defined as a perception that tobacco use is harmful or undesirable (less attractive, less comfortable in public gatherings), while a “positive attitude” indicates a more favorable or accepting view of tobacco use (more attractive, more comfortable in public gatherings). Sadly, 65.4% of Congolese adolescents aged 10–17 years have a positive attitude towards tobacco and nicotine products.7 In other words, more than half of the adolescents find tobacco use attractive and comfortable to be used in public.Attitudes toward tobacco use among adolescents aged 10-17 years in the DRC
Source: DaYTA DRC (2024)
More than half of the adolescent population aged 10–17 years in the DRC find tobacco attractive and comfortable to use in public, no matter the sub-category considered.
Disaggregation of attitudes toward tobacco products among adolescents aged 10-17 years in the DRC
Source: DaYTA DRC (2024)
Perceptions about tobacco products by adolescents in DRC
According to the DaYTA study,
adolescents’ perception of tobacco products in the DRC include views on attractiveness, comfort, safety, and the perceived cost of cigarettes. The concept of perception captures how adolescents feel while consuming tobacco and nicotine products. Overall, about 30% of Congolese adolescents believe tobacco enhances attractiveness, with boys slightly more inclined (31%) than girls (27%); while 27% think it makes one less attractive (girls 32%, boys 25%). Regarding safety, 26% agree that tobacco is safe for short-term use if one quits later, and only 10% consider it safe overall—boys being more optimistic (28% and 13%) than girls (21.2% and 4.3%). In terms of comfort, 25% feel tobacco increases comfort (28% of boys vs 20% of girls), though 40% believe it reduces comfort (41% of girls vs 39% of boys). Adolescents estimate the cost of a pack of 20 manufactured cigarettes at about 2206 Congolese francs, with boys perceiving it slightly higher than girls. Lastly, while 57% recognize the harm of secondhand smoke, this concern is more marked among girls (63%) compared to boys (44%).Summarily, irrespective of the perceived view, more boys than girls perceive the use of tobacco and nicotine products as attractive and beneficial.
Perception of tobacco products by adolescents aged 10-17 years in the DRC
Source: DaYTA DRC (2024)

Marketing of tobacco and nicotineproducts
On one hand, adolescents in the DRC are exposed to pro-tobacco media messages through various sources. Among those exposed, 41% saw someone using tobacco on TV, 24% saw someone using it on social media platforms, and 17% encountered advertisements or promotions at the point of sale.
On the personal engagement side, 51% said they would wear something bearing a tobacco company or product name, and 9.7% had ever been offered a free tobacco product. Overall, both boys and girls exhibit similar exposure trends.Exposure to pro-tobacco media messages by adolescents aged 10-17 years in the DRC
Source: DaYTA DRC (2024)
On the other hand, 15.5% of adolescents reported encountering anti-tobacco messages through traditional media channels—such as television, radio, internet, billboards, posters, newspapers, magazines, and movies—with a similar exposure percentage for boys (15.2%) and girls (16.1%).
Additionally, 10.2% of adolescents reported seeing anti-tobacco messages on social media platforms, with slightly higher exposure among boys (10.7%) compared to girls (9.1%). This shows that media play an important role in influencing positive and negative trajectories of adolescents consumption of tobacco and nicotine products in the DRC.
Cessation
Overall, 63.5% of adolescents in the DRC who were tobacco users reported that they had not received any tobacco cessation support in their lifetime.
The DaYTA study also found that tobacco cessation programs and professionals do not provide enough support to adolescents willing to quit tobacco in the DRC both during quit attempts (4.7%) and throughout their lifetime (2.7%). This could be explained by the very few number of cessation programs and professionals in the country, and especially by the lack of financial support from the Congolese government for grassroots anti-tobacco activities.Overall, 23% of current tobacco users are seriously thinking of quitting, with boys taking the lead (26.5%) over girls (17.4%). Many reasons are put forward by the youths to quit tobacco. Among the reasons for cessation, improving health is the most commonly cited motivation, with 30% overall—34% of boys and 22% of girls indicating this reason. Saving money is another factor, reported by 13% overall, with 14% of boys and 11% of girls. Notably, family disapproval plays an important role, especially for girls, as 29% overall cited it, including 24% of boys and 39% of girls. A smaller percentage mentioned that they would quit because their friends do not like tobacco use (3.9% overall; 4.2% of boys and 3.2% of girls), and 15% indicated that they would stop simply because they wanted to (14% of boys and 18% of girls).Reasons for cessation of tobacco use given by adolescents aged 10-17 years in the DRC
Source: DaYTA DRC (2024)
Most Congolese adolescents think it is quite easy to quit consumption of tobacco and nicotine products. In the context of quitting tobacco completely, 33.9% indicated it was very easy and 22.3% found it very difficult. Notably, girls reported higher ease in both scenarios (42.8% and 15.5% for “very easy” and “very difficult,” respectively) compared to boys. Regarding support during their most recent quit attempt, the vast majority (67.1%) tried to quit on their own, with only a small minority receiving help from professionals (4.7%), friends (13.6%), or family (13.8%), and even fewer used medication (2.4%). Lifetime support was similarly limited, with 63.5% reporting no support, a figure higher among girls (69.3%) than boys (60.6%).

Overall reflections and policy recommendations

Legislative and regulatory measures
- Monitor and penalize violations, particularly near schools and youth-dense areas.
- Include new and emerging tobacco and nicotine products (e-cigarettes, nicotine pouches, shisha, etc.) in tobacco control laws.
- Require tobacco companies to import only cigarettes with graphic color photos on the packaging (burned lungs, mouths wide open with rotten teeth, feet with amputated toes, etc.).
- Strictly prohibit the depiction of tobacco in cultural works, including shows and films, particularly the depiction of characters smoking.
- Help farmers and farm workers convert from tobacco cultivation to sustainable food crops.
- Run an anti-tobacco mass media campaign as required by the WHO.
Restrict access to tobacco for minors
- Strictly enforce age restrictions on tobacco sales, ensuring penalties for vendors who sell to minors.
- Prohibit the sale of single cigarettes and small packs, which make tobacco more affordable and accessible to adolescents.
- Regulate and monitor the sale of tobacco through vending machines and online platforms to prevent underage access.
- Require identity cards verification and impose fines for illegal sales to minors.
Tobacco taxation
- Substantially increase excise taxes on tobacco products to make them less affordable to adolescents.
- Ratify the protocol to eliminate the illicit tobacco in the country
Health education and awareness
- Develop and implement comprehensive youth-focused anti-tobacco campaigns that highlight the health risks of tobacco use.
- Integrate tobacco education into school curricula, emphasizing the dangers of early initiation and dispelling myths about “safe” tobacco products.
- Promote collaboration between the Ministry of Health and the Ministry of Education to adapt the health education curriculum to the context of increasing tobacco and nicotine consumption by adolescents.
- Promote youth-led campaigns to challenge the social appeal to tobacco use.
- For out-of-school adolescents, establish community-based educational programs and peer-led interventions in collaboration with local organizations, youth centers, and healthcare facilities, ensuring that prevention messages reach this vulnerable group.
- Engage community leaders, parents, influencers, and teachers to promote non-smoking norms and prevent peer influence especially in rural areas.
- Include graphic health warnings on packaging in local languages for adolescents in rural areas.
Youth support and cessation services
- Establish youth-friendly cessation programs, including counseling and behavioral support in schools and healthcare centers.
- Train healthcare providers and educators to identify at-risk adolescents and offer interventions for tobacco cessation.
- The Ministry of Health should introduce a toll-free number for assistance 24/7.
- The Ministry of Health should facilitate drug distribution and reduce detoxification costs for those quitting.





